Fascia and acupuncture: scars
- Simon Bélair

- Jan 14
- 4 min read
Updated: Jan 22
Wound healing is a fascinating process. It involves a dynamic interaction between the migration, proliferation and differentiation of different cell types, the expression of cytokines and growth hormones, the synthesis and remodeling of extracellular matrix components, as well as many other complex interactions (Shleipp 2020).
Wound healing occurs in four phases: bleeding, inflammation, cell proliferation, and remodeling. Although remarkable, this mechanism sometimes leaves sequelae in the form of densification, adhesions, or fibrosis, which lead to biomechanical, circulatory, and sometimes even emotional consequences.
How can acupuncture help mitigate this process? What techniques are best suited for specific cases? How can local needling can have in impact elsewhere in the body?
Scars and fascial restrictions
Fascial restriction is described as any obstruction to optimal gliding, at both macroscopic and microscopic fascial organizational levels, between endofascial fibers and interfascial planes. Such restriction can cause tension abnormalities and movement disorders (Fourie 2008). Short-term fascial restrictions affect tissues locally, while long-term restrictions induce a more global pattern of dysfunction (Langevin 2006).
Fascial tissue is involved in the exchange of bodily fluids and the coordination of mechanoreceptors. Decreased fascial mobility can impair blood flow and cause ischemia, thereby deteriorating the quality of muscle fibers (Vaticon 2009). Since many mechanoreceptors are embedded in the fascia, impaired proprioceptive input can alter the tonic contraction capacity of optimal muscles (Vaticon 2009). It is generally assumed that the tissue shortening and stiffness observed in these pathological conditions are caused by myofibroblasts (MFBs), and that the resulting tissue contraction is achieved through a progressive combination of cell contraction, collagen cross-linking, and matrix remodeling (Tomasek et al., 2002).
Acupuncture has demonstrated surprising results in its ability to remodel the extracellular matrix and its fibroblasts and to reorganize collagen fibers into parallel and ordered bundles.
Acupuncture, fibroblasts and collagen
Fibroblasts are the main type of cell in connective tissue and play an important role in wound healing (Qian et al. 2022). Acupuncture has demonstrated surprising results in its ability to remodel the extracellular matrix and its fibroblasts (Langevin 2003) and to reorganize collagen fibers into parallel and ordered bundles (Xiong F et al. 2025).
The Huáng dì nèi jīng describes a total of 26 needle techniques. There are techniques for every type of tissue, and many are very useful in treating fascial dysfunctions. Manipulating the acupuncture needle can indeed cause a lasting change in the extracellular matrix surrounding the needle, which can in turn influence the various cell populations sharing this connective tissue matrix (e.g., fibroblasts, sensory afferents, immune and vascular cells) (Langevin and Yandow, 2002).
Case studies
Here are two typical examples of scars treated with knowledge of fascial anatomy and physiology, in accordance with the treatment principles of Huáng Dì Nèi Jīng . In both cases, palpation is central to the choice of puncture sites and techniques used.
Case #1:
Woman, 50 years old
Triple fracture of the medial malleolus 12 years ago during a skating accident.
Pain and swelling in the legs and thighs. Restless legs syndrome.
Sensitive, red scar, adherent to the periosteum.

Observation and summary:
The scar (still active) prevents the proper venous and circulatory functioning of the yin meridians of the leg as well as impeding proper nervous transmission.
Therapeutic strategy:
The puncture (26G, 2 cun) aimed to release adhesions between the crural fascia and the periosteum at the level of the medial malleolus. The evolution of the scar over a period of 3 weeks can be seen. The reduction in symptoms was significant and gradual over 1 month.
Clinical explanation:
As mentionned in the book : Scars, Adhesions and the Biotensegral Body, by Trewartha and Wheeler:
''Sometimes, in the course of healing, one fascial sheet will stick to another, causing adhesions that bridge a superficial to a deep “layer”. For example, in a compound limb fracture, the periosteum of the bone may become fixed to the overlying skin, and the scar will be thin and hard (and often tender), tethered to the underlying bone. Small nerves are often severed in laceration injuries and, in the course of wound healing, regrowth may result in painful, bunched up bundles of knotted nerve endings in the scar called neuromas.''

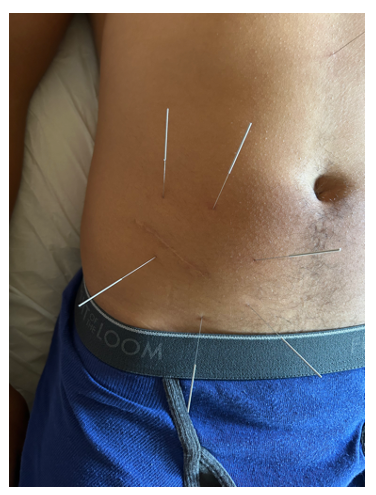
Case #2:
Man, 45 years old
Appendectomy scar since 2010. Lower back pain since then without improvement from local and regional treatments of the posterior chain.
Observation and summary:
Post-operative scar that prevents the sliding of the abdominal aponeurosis and the proper functioning of the thoracolumbar fascia.
Therapeutic strategy:
Puncture (30G, 1.5 Cun) of local and peripheral scar tissue to restore the gliding planes of the abdominal aponeurosis and thoracolumbar fascia expansions. Significant reduction in back pain is observed from the first session. Note that the needle placement is not necessarily very close to the scar. The visible scar does not always correspond to the internal damage and compensations of the connective tissues. It is therefore important to develop palpation skills to follow the direction and the depth of the adherances and fascial dysfunctions.
It is therefore important to develop palpation skills to follow the direction and the depth of the adherances and fascial dysfunctions.
Clinical explanation:
Abdominal scars, due to the fascial and muscular restrictions they cause, can have a major impact on the biomechanics of the trunk and are an underestimated cause of chronic back pain. By altering the sliding of the abdominal aponeuroses and functional continuity with the thoracolumbar fascia, these restrictions disrupt the distribution of tension, the transmission of forces, and proprioceptive afferents, promoting the onset of low back pain that is sometimes resistant to local treatment (Stecco, 2015).
Conclusion
Scars are much more than just a mark on the skin left by a past event. They are areas of deep tissue remodeling, capable of inducing lasting fascial restrictions, circulatory disturbances, and neurosensory alterations that can manifest locally or remotely.
Acupuncture, through its direct mechanical action on connective tissues and the extracellular matrix, is a relevant approach in the treatment of pathological scars and on their structural and physiological consequences. Anatomical and physiological knowledge of fasciae, as well as palpation skills, play a central role in choosing the location of puncture sites and the techniques used.



Comments